The Neurology of Movement – Unilateral vs Bilateral (II)
The Neurology of Movement (continued)
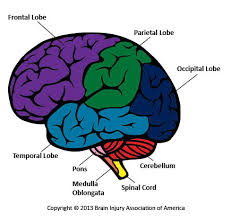
- Cerebellum – integrates (and simplifies) the complex data generated from all of our body systems and cognition. Important: it is involved in balance of the body. The cerebellum performs several tasks in movement, such as:
- Coordinates complex movements ispilaterally (occurring on the same side of the body);
- Is in direct communication with the ipsilateral vestibular system;
- Directly stimulates the contralateral cerebral cortex (frontal lobe).
- Frontal lobe – contains the primary motor cortex which controls voluntary movement and specific body parts.
- PMRF (Ponto medullary reticular formation)– having the role to:
- Inhibit pain of ipsilateral side of the body;
- Inhibit the ipsilateral IML (Inter Mediolateral);
- Inhibit the ipsilateral anterior muscles above T6 (thoracic vertebrae); inhibit the posterior muscles below T6;
- Inhibition of inhibitory Motor Interneuron (Renshaw Cells).
About 90% of the signals that go down to the body from the cortex go through these nuclei of the PMRF.
The cortex is sending information down the rest of the body through the Sympathetic Nervous System (a division of the Autonomic Nervous System), responsible for blood pressure, oxygen saturation, posture, muscle tone, etc.
Understanding the Neurology of Movement:
- Healthy, strong movement requires healthy, active neurologic signalling;
- If deficits exist in the cerebellum, cortex or PMRF then movement and strength suffers!
Exercise ramification:
When you do movement with your left hand, all that information (signal) goes to your left cerebellum and activates it. Left cerebellum sends information across the brain to the right cortex. The right cortex is going to fire down into the right side PMRF (which is responsible for inhibiting pain, improving muscle tone, helping posture, etc)
- Screen the cerebellum to establish a “likely” starting point;
- Use practical intra session assessments to see how your client is responding to the exercises;
4 practical intra-session assessments:
- Active Range of Motion (AROM);
- Strength – RPE (rate of perceived exertion) from 1 to 10;
- Balance (15 seconds);
- Functional Activities (Sports or ADL);
AROM:
- Shoulder flexion (arm to front);
- Shoulder abduction (arm to side);
- Shoulder extension (arm behind);
- Trunk forward bend;
- Trunk rotation.
Bilateral vs Unilateral Testing Protocol
Assessment 1: cerebellum (upper body, lower body, toe taps);
Assessment 2: (choose from the following): AROM, strength, balance, and functional activity;
Perform 1-2 Test Reps Bi & Uni: vertical push, vertical pull, horizontal push, horizontal pull, squat pattern, lunge pattern;
Re-Assess: good response – continue to set; poor response – choose different version of exercise.
Neurology of Movement
Take home message:
If the deficit had a neurologic cause and not a biomechanical one, then bilateral exercise is not the answer as it may decrease range of motion and may make everything worse.
Keep an open mind and approach this as a scientific experiment.
Try one full training session on yourself to see how it feels and what you learned.
I am definitely going to do it.
*https://www.youtube.com/watch?v=b5R5Qk76o_c&feature=youtu.be
*Exercise Physiology – Understanding the Athlete Within – The University of Melbourne
*Synapses, Neurons and Brains – Hebrew University of Jerusalem
*Photo – Brain Injury Association of America